|
Growth charts! They are a huge topic, partly because of many opinions on them. There are good reasons why there are so many opinions on them. One thing to keep in mind, believe it or not, is that they are not all the same. The growth chart I use vs the one some doctors use vs public health vs all the apps is that some use older versions that were made and provided by formula companies, some use the CDC, some use the WHO, and some maybe even have their own.
Once upon a time, I was trained to not really consider what growth charts said because the ones we had were made in the 1970s/1980s with a group of all American Caucasian formula fed babies and they were distributed to health care providers by formula companies. Because of this, it was believed they had no relevance to breastfed babies. This isn't entirely wrong, but this is also no longer the case. The growth charts available today have since been redesigned. The WHO one is now based on breastfed, world wide babies with much more detailed analysis. I will point out there are many growth chart versions available - so please look to see what is being referenced. With proper understanding they can be a very useful tool and tell *part* of the story of growth. The WHO developed standards of growth of the breastfed infant as the norm for growth. The WHO charts reflect growth patterns among children who were predominantly breastfed for at least 4 months and still breastfeeding at 12 months. In contrast, the CDC growth charts are references. They identified how typical children in the US DID grow during a specific time period. Typical growth patterns may not be ideal growth patterns. I often say "just because something is common, does not mean it is normal." The WHO growth charts are standards; they identify how children should grow when provided optimal conditions. The WHO standards are based on a high-quality study designed specifically for creating these growth charts. For the CDC growth charts, weight data were not available between birth and 3 months of age and the sample sizes were small for sex and age groups during the first 6 months of age. There are lots of gaps in these charts! Some infant apps actually use their own version! It is still common to hear statements like “don’t worry about it” but sometimes this is secret code for “I don’t know how to help you” or “I don’t know how to read the data” or “I don’t understand what the chart is telling me”. I get asked about infants stooling patterns quite a lot, typically from worried mothers who have an infant who has slowed down on stooling, maybe 1-2 days, sometimes 7-10 days. The baby might also be gassy, not sleeping or fussy. Moms often will ask various sources if this is normal or expected. I was certainly taught to believe this with a variety of reasons as to why. As an IBCLC I don’t consider this to be normal, anymore, and I will list some of the reasons as to why later. In my opinion, the information I had been provided over a decade ago is still how health professionals and peer support are being taught in their education and orientation to units and job positions that support infants and mothers is also teaching this way. The number one reason I hear is that breastmilk is just highly digestible & there is nothing left to dispose of. My common sense response to those who say ‘it’s just absorbed’, is why then when babies finally do have a bowel movement is it always reported as “a huge blow out” or why do babies have “poop days”. The days are described as days where, once the stooling starts, it does not stop for several diaper hours. If it was readily absorbed, it wouldn’t be an explosion or take hours to clear out the bowels. In recent years more information has come out to tell us that, in fact, there are known constituents in breastmilk that are not digestible. One specific component is human milk sugars that are attached to the lactose molecule in breastmilk. They can make up to 20% of the content of milk. So, to think that ⅕ of the intake of what an infant consumes is not digestible, makes one wonder where it goes. It appears though, that this doesn’t have a role in nutrition, but instead in gut health. The bacteria of the infant gut is what thrives on these human milk sugars, not so much that an infant's growth thrives here. This could be one of the reasons why we may often see a baby gaining weight well, but not be stooling. But we might see a colicy or gassy baby, because the gut flora isn’t quite ideal. I find often getting more milk into the baby helps these symptoms. More milk = more human milk sugars = more healthy bacteria. Not to mention other little things that end up in stool. The process of digestion alone would have some sort of byproduct left, even just the epithelial cells of the digestive tract sloughing off along the way.  Baby not pooping? 3 days? 10 days? Is this normal? I stated the number one reason that I hear as a reason why babies might not be stooling is that people believe breastmilk is digestible and I have provided some reasons as to why this is not true. But, I am actually more concerned about another aspect of the non-stooling situation, beyond just human milk sugars and bacteria content. I have shown my belief of *if milk is going in, stools need to be coming out”. When I come across a non-stooling infant, I want to have a look at the growth patterns of these infants. I mentioned thriving infants above because it is very important to discuss infant weight gain in all of this. Watching just pee alone is dangerous as babies can get to a pretty scary place before they start to really slow down on the peeing and may be in a state of failure-to-thrive at that point. We can possibly avoid that by watching stooling. I will say it one of the first signs of lower than required intake in many many babies I have worked with. This can all actually have a long term effect on breastfeeding. As babies take in less milk & have slow or no weight gain , milk supply can be lowered, resulting in even less milk being taken in by the baby and the cycle continues. It can also be a sign of more going on and the sooner we intervene and assess the situation, the sooner we can strategize solutions to prevent things from a downward spiral. What should we expect in a babies diaper then? This is what I recommend. As babies get closer to 4 months, they may slow down to 2-3 diapers a day, but in the early days and weeks fore sure with each good feed or couple feeds, there should be a bowel movement. 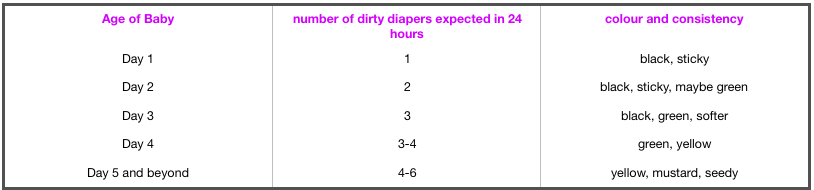 I also want to mention that these ideas and supporting information is quite new, so just like we have to be patient with babies and how they grow and change and develop, we have to be patient with the research and learning of the changes and developments coming out in breastfeeding. As much as we have been breastfeeding “forever”, it was a time before so much evidence and research existed and was desired.
If you are concerned about your babies stooling patterns, I am always happy to help explore that with you. I welcome you to reach out for a consult, in person or virtually. (originally posted Feb 21...I am sure more will be added as time and linked thoughts come up)  If I asked myself if pumping was being used as a magic fix for common, yet easily managed, breastfeeding concerns I would have to say "yes, it is". The idea to pump instead of, or in conjunction with, breastfeeding is often suggested to mothers by their support people. These support people include other new mothers and experienced mothers at places like Mommy and Baby Yoga, Mommy and Me time, Kinder Music, Baby Signs, the museum, StarBucks, online support groups, mommy chats, any place mom's and babies hang out together; you all know where mommy's go. Other support people are their mothers and mother-in-laws, sisters, sisters-in-laws, aunts, grandma's, that old family friend; again, you know who these people are. Of course, other new mother's support people include Health Care Providers like doctors, nurses, midwives and the complementary support people like doula's and childbirth educators. And, in case you are not aware, these people include many that did not breastfeed themselves or were not successful in their attempts to breastfeed.
Most new moms have the intention of breastfeeding, as so as expected, it comes up in conversation. People feel the need to ask new moms how breastfeeding is going, new moms feel compelled to seek out support in these early weeks or health care providers are following up mom and baby. When moms are asked about breastfeeding they share the concerns they have with breastfeeding in hopes that someone can help them. Here is the list of common complaints and one likely answer they will receive to alleviate that concern. Sore Nipples -> Pump and bottle feed Baby not effectively sucking -> Pump and bottle feed Thrush -> Pump and bottle feed Engorged -> Pump between feeds Plugged Duct -> Pump between feeds or pump and bottle feed Needing to feed in public -> Pump and bottle feed Over Active Let Down -> Pump before feeding Low supply -> Pump between feeds or after feeds Baby not sleeping -> Pump and bottle feed or have someone else feed Colic -> Pump and have someone else feed Foremilk/Hindmilk concerns -> Pump before feeding It appears that pumping can be a common suggestion to alleviate the most probable breastfeeding issues. We need to be aware it is not a magic fix, it is most likely to be a band-aid, and it does not "fix" anything. We also need to be aware that pumping can create more issues. These are just a few ways this pumping band-aid could create more issues for mom and baby. With sore, bleeding, cracked nipples, generally the most common concern, generally easy to fix, pumping only results in double the work. Why would a new mother want to add in all the extra work of pumping and bottle feeding when getting some assistance with position and latch could make the problem go away, in even the very next feed? Or one of the many other solutions with have to help with the pain and healing. Often long term pumping is not going to sustain a babies needs and milk supply like breastfeeding directly from the breast would. Often breastfeeding relationships end far sooner than mother's intended due to supply issues because it leads to supplementation or another feeding method all together. This might not be the case all the time, as some mothers, do exclusively pump, but there is unique difference between a mother who makes the decision to exclusively pump compared to one who is trying to get baby nursing pain free at the breast and needing to pump in addition to. How about that baby that just is not sucking effectively or will not latch? Let's see, how do people learn? We learn by doing. If we take baby away from the breast, how does he learn? Again, we need to support moms and babies in positioning and latch and innate instincts that babies have to feed and let them learn together. If habitual placement is still not getting baby latching and sucking, we need to further evaluate what might be going on with that baby. Ignoring the difficulty baby is having and turning solely to the pump does not make the original issue baby was having go away. Thrush is no reason to stop feeding at the breast. The reality with pumping with thrush is that mothers now have more parts and equipment to treat or throw away. Thrush can sometimes take time to clear up but it spreads so easily, we need to restrict what comes into contact with the thrush to stop the spread of it, not add more to it. There are medication and alternatives that we can use to treat thrush and the discomfort of thrush as we are trying to eliminate the nasty little bug it is. Milk supply works on supply and demand so as well as pumping to relieve engorgement seems like a good idea right now, later on the fullness comes back and generally more full then the previous time, as a mother's body thinks that is milk that baby needed. If moms are engorged because a baby is not eating or draining the breast, then the answer is to get the baby eating and draining the breast, not pumping. The more baby is at the breast the less engorged mother's will be, assuming baby is eating well. Again, back up to latch and sucking. If baby is not waking to feed and mom is starting to fill up, mom can put baby to breast and encourage that baby to eat, to play his role in this breastfeeding relationship. Another concern with engorgement is that as much as it may seem logical that when mothers are engorged, it means they have a good, healthy milk supply, in fact the opposite can occur. The more often a women is engorged, the faster her milk supply will start to decreased. When breasts are full it sends a signal to the part of moms brain responsible for milk supply to slow production down and milk making cells start to shut down, resulting in less milk in the days ahead. Pumping when engorged can also pull more fluid, and not just milk, into the breast, resulting in edema. Often that fullness or edema is confused for milk and "good supply". Plugged ducts are uncomfortable, in fact down right painful, and yes moms want them out, but pumping is not the most effective way to unplug a plugged duct. In fact it can lead mom right back to the engorgement stage and create the spiral onwards from there, when the easiest way to get rid of that plug is by using baby, again, or some other strategies that are much more effective. I am starting to see a larger amount of women pumping so they can feed their baby while out and about. First, people that want to go out in public just need to accept that mothers and babies go out in public, too, and mothers and babies use breasts to feed. Secondly, mothers need to be informed about how this "solution" really is only one that is feasible for a small time. Each feed mom misses at the breast impacts that supply and demand mechanism again. If mom is out and is not feeding baby or replacing a feeding session without pumping again her body and brain communicate this to each other and the process of milk supply slows down. This again goes back to what I mention early about keeping up supply, supplementing and ending the relationship early than expected. Over Active Let Down is a problem that some moms struggle with but again pumping can just aggravate this problem. It is an easy problem to aggravate as it can lead to the engorgement issue and when baby is ready to feed, mom is ready to burst with milk and when the let down occurs it is like opening up a dam. Baby gets flooded with milk, has trouble managing flow, staying latched, becomes upset and this all causes frustration in mom and baby. Positioning, latch and frequent feeds are the easy fix here. On the other side of it, some babies have a hard time handling a normal let down, but it mimics and over-active let down. We need to be sure that we know if we have a baby that is struggling with a normal flow or a true over active let down. Another strategy I will mention here is block feeding. Block feeding used to be a common strategy for overactive let down but in more recent years, we have come to learn this is often detrimental to breastfeeding, as well. It appears to create a downward spiral of low intake, low weight gain and low milk supply. Always have what appears to be an overactive let down assessed by an IBCLC. For the healthy, full-term infant pumping for perceived low supply should be the last resort. Babies truly are the best solution here again; baby to breast = more milk in breast. Secondary low milk supply is a different issue and does not fall into the category of common yet easily managed breastfeeding concerns., which is what I am addressing here. I am also not addressing primary low milk supply which are maternal factors in less than 5% of mothers who do not make enough milk. These conditions should be determined with through evaluation with an IBCLC and primary health care providers. I am talking about common breastfeeding concerns that most mothers face. Pumping to top up or to force more milk into that non-sleeping baby:. Fuller tummy does not equal more sleep in babies. Babies have very small tummies, breastmilk is readily absorbed and digested so babies feed frequently. The issue here is not the amount of milk the baby takes, but rather unrealistic expectations and misunderstandings babies. If babies are really struggling with sleep, it is worthwhile seeking out a feeding assessment to ensure all the things above are not an issue. If baby is not gaining weight well and is also struggling with sleep, this is a different story. Colicky babies are much better soothed at the breast than any other way, pumping to feed another way removes that comfort source from this already high needs baby and can make the baby even more upset. There is no real understanding behind colic and why some babies are colicky and some are not but there is good understanding that skin-to-skin and mothering at the breast calms these babies best. Again, all things above should be ruled out before we just assume we have a colicky baby. I have also come to believe colic is an umbrella to other providers. I think sometimes we can seek some clarity on these babies and get past colic, rather than waiting it out. If you have what appears to be a colicky baby, perhaps booking for a breastfeeding session will give some of that clarity. Foremilk/hindmilk imbalance or what is being perceived as such seems to be rampant these days. It seems like a viral condition that has spread. So many moms seem to feel they have this issue, when in fact it is very rare. However, if a mother thinks this is an issue she has and pumps to get to the hindmilk, we go back to the engorgement cycle where mom has too much milk, can have a forceful let-down and then babies do get more foremilk than hindmilk, they are upset by the flow of milk and we end up in a vicious cycle. Worst case scenario, in fact, this could create that colicky baby we all fear. Foremilk/ hindmilk is best controlled by frequent feeds, proper positioning, good technique, etc. Mom's please seek out appropriate, knowledgeable, support when you encounter these easily managed breastfeeding concerns. “You need to nurse for 20 minutes on the first side and then move baby to the other side for twenty minutes.” or "You have to empty the first breast before going to the second breast". Did anyone ever tell you these things? What if your baby only nursed for ten minutes? Did you ask what would happen? I suspect you may have been told that is not long enough for your baby to get the hindmilk (higher fat milk). Is 20 minutes that magic “long enough” time frame? What if baby wanted to be there for 25 minutes? What happens then? Do you have no more milk?  Are you breastfeeding and feeling like you have to watch the clock? How about we focus on watching the baby and take cues from them about what they need. Have you ever expressed breastmilk? What does it look like? Have you expressed more than one time? Did your milk look the same each time? I suspect it varied from thin, watery and blue, to yellow and thick. Did you notice a difference with the time of the day you pumped? How about before a feed or after a feed?
What does the research say? In point form the basics are: · As the baby feeds the content of the milk the baby receives is higher in fat · Each feeding can vary in fat content over the course of the day · The fattiest part of one feed might actually contain the same fat content of the start of another feed · Milk is milk; no real need to differentiate foremilk and hindmilk. Some is more concentrated, some less so, but your baby needs it all.(Hindmilk would be better called "concentrated milk" and foremilk "dilute milk") · Babies all stay at the breast for different lengths of time and what satisfies them varies · The breast is not a reservoir. It is never “out” of milk. If babe hangs out nursing more milk will “let down”. If you switched breasts milk may flow faster because more milk is in that breast, but there is no rule to have to take a baby off one side to put him on the other because of foremilk and hindmilk. Yes, if we want "moremilk" Is there a time when we might pay more attention to foremilk and hindmilk? · Is there an issue with baby sleeping at the breast? · Is there an issue with baby being fussy at the breast? · Is there an issue with babes weight? · Is baby swallowing at breast? · Is baby relaxed, with wide open hands and content at the end of feeds or no? If there are any of these types of concerns, seek out an IBCLC to address the concerns. It may be somewhat related to the so called foremilk/hindmilk. It can sometimes be ONE factor to take into account for the whole picture when some of the above issues are seen. But it would not solely be a foremilk/hindmilk issue. When a woman plans to breastfeed her baby and that plan doesn't go accordingly, it can be a time of many emotions. This emotion is often referred to as "guilt". There is a common saying, "we shouldn't make women feel guilty for not being able to breastfeed." Of course, we shouldn't. There are so many factors, however it is not a black and white, can or can't, choose to or not, it works for some, not for others, etc. "Don't make her feel guilty" I don't want a mother to feel guilty, but I do want her to recognize her feelings about her situation. Feelings are not negative. Feelings are just feeling. And we need to feel to work through the struggles. We need to explore the feelings women experience when it comes to feeding their infant. Everything we see now is "Breast is Best". We have become a society that is "great" at encouraging breastfeeding but we are not a society that is even "good" at supporting and sustaining breastfeeding. This means many women are not meeting their breastfeeding goals. With that comes many feelings. Mothers who intended to breastfeed but struggle to meet that goal, feel a sense of loss. We know there is a connection to loss of breastfeeding and postpartum depression. We need to recognize that many mothers experience grief, and not guilt, in the postpartum period. I feel like grief is confused for guilt or a feeling of failure and it is not interchangeable. Mothers need to be given the opportunity to grieve what they had planned, what they believed postpartum would be like, the support they would receive but did not. Hearing “now, now dear, it’s ok, formula feeding is ok” doesn’t really help. It doesn’t help because it is not about breastmilk over formula. It’s about an expectation mothers had. It’s about a decision they thought they had control over, only to find out breastfeeding is difficult, but more so motherhood is difficult! It is all more difficult than society lets people believe. Breastfeeding is not well supported. It is not understood well. So many myths and wise tales still exist and are perpetuated daily, holding women back.  Women are finding themselves alone, feeling isolated & without reliable resources. Women who choose formula from the start don’t feel this way because they got to make that choice consciously. Women who planned to breastfeed but missed out on proper supports don’t feel like they had any other options but to give up their plans to breastfeed. That’s not a choice. That’s survival. We need to guide mothers to the appropriate, breastfeeding educated resources in a timely manner. Mothers deserve to have choices, someone who can offer solutions that are acceptable to them & who can provide support and counsel when breastfeeding isn't the best option for them.
Many mothers will be able to relate to this experience. The experience looks the same; a routine infant check up appointment, baby gets a weight check, the parents are asked some questions about development, etc. Upon looking at the weight, it is determined the infant is not gaining weight as expected. What does this mean? What is the cause? What should be done? It often is quite shocking to parents, especially mothers, to hear this news. They are perplexed because they thought feeding, usually breastfeeding, was going ok. How is it possible that baby isn’t gaining weight? How is it possible she didn’t know that baby wasn’t growing as expected? Can anything be done?  Common reasons provided for this phenomena is that mom has low milk supply, baby isn’t getting enough hind milk or baby is too sleepy and isn’t feeding often enough. I don’t think it is quite that simple.
What I find in these scenarios, because I get calls often after an experience like this, is that what is not communicated to the parents is why we do these checks, why they matter, what they mean and what should be done with the information. The simple answer is that we expect babes to maintain their own curve that they plotted on at birth (or more ideally 24 hours). When babies start to drop off that curve, this gives us a sign to look and assess what might be happening. This is a clue to ask some more questions and see if there are other pieces that can help tell us what might be happening. We want to know more about feeding behaviour, mood, output. Often what I hear is that there is no way baby needs to eat more. They are happy, content, sleep well, don’t really fuss. The opinion is that there is no way it is possible the baby isn't eating enough. People expect a hungry baby to cry, be irritable, to unsettled. I am going to say this is simply not true. I am sometimes more concerned about that “good baby” that sleeps well and always content. A very misunderstood piece of infant wellbeing is that weight gain influences appetite. What I mean by that, is that if a baby is gaining well, they demand to fed and show signs of being hungry regularly with easily identified feeding cues. What we think is a content baby because they have a calm mood, could be a baby who is content but not getting quite enough intake. A baby that is lower weight than expected, will have a lower appetite and will in fact cue less to be feed, will have subtle cues, likely won’t have a late hunger cueing & overall may make little fuss about it. If mother offers they will feed, but commonly have short feeding sessions. When they are being feed, their appetite is low so they do not do an efficient job, leading to milk being left in the breast and the body slowing down production. I give the example that if they are getting 70% of their intake requirement, they will eat at 70% efficiency (this will very baby to baby). This over time can cause a low supply, which influences their feeding because babies like flow...so low flow, means less interest in feeding and the cycle continues. If none of that concern is explained to a family, they leave these routine visits confused and bewildered as to why some one had a concern or what they could/should do about it and have no idea why it happened in the first place. There are lots of factors to consider to understand why this is happening & what the appropriate action for each case should be. If you are experiencing a difficult feeding situation where weight gain is a concern, booking a consult with an IBCLC is advisable. With a good assessment by an IBCLC, the root cause can often be determined and a solid plan can be put into place to get the baby fed, get weight gain concerns addressed, increase milk supply, maintain breastfeeding, etc. Other things to note in cases of lower than expected weight gain could be:
Has someone suggested to you that your baby isn't gaining weight as expected and the solution is to get baby to ingest more hindmilk? It has become common knowledge that fat content of milk changes throughout breastfeeding. This is true. Milk doesn't change in each feeding session in the same way...it changes over the course of the day and feeding patterns. The anxiety about whether or not baby is feeding "long enough" to get to the hind milk is not necessary.  Something else that is true is that the longer a baby feeds, the more letdowns occur and more fat is released into the milk from the milk making glands, however...there are some things that need to be pointed out and kept in mind.
Foremilk and hindmilk are not two different kinds of milk. Women do not produce a low fat milk and a high fat milk. It is simply that the first milk a baby receives at the start of a feed is *fore*milk and the milk after that is *hind*milk; in a way meaning initial milk and subsequent milk. The change is gradual It is not based on a percertange of fat content, like skim, 1%, 2% or whole milk that we are used to thinking of. There is no magic time in a feed that changes the fat content or we can see a switch of kind of milk. There is no percentage of fat a baby needs to be able to gain wright. On this note, all the foremilk is not always lower fat than all the hindmilk. Foremilk from one feed might have a higher fat content than hindmilk from the next feed, previous feed or other feeds in the day. With this all in mind, when there is a weight gain concern, the focus needs to be on increasing intake of milk and looking at the factors that might be impacting intake & not trying to avoid foremilk. Strategies to avoid formula and increase hindmilk consumption are ideas like pumping foremilk before a nursing session, so baby can only access hindmilk or keeping baby on one breast for 15 or 20 or 40 minutes, depending on who is giving the instructions. In fact, sometimes these strategies means the baby is getting even less milk than before. It is the total daily milk intake that determines successful weight gain. We cannot look at one feed as the way it is for all feeds. We need to look at each day and all the breastfeeding sessions combined and then address ways to increase milk intake overall. I wrote about this again in another post; you can read that here. If you find yourself in the situation of having an infant that is not gaining as expected, not gaining at all, slowly gaining or losing weight, I suggest a full evaluation with an IBCLC. |
Kim Smith
|
 RSS Feed
RSS Feed

|
|
Quick facts:
International Board Certified Lactation Consultant (2010), Re-certified (2015, 2020) TummyTime Method Instructor Retired Doula, CAPPA trained, Pre-Certified ProDoula (2009) Your Birth Experience (YBE) Certified (2015) Wife & mother of 4 Retired Medical Laboratory Technologist |