 If I asked myself if pumping was being used as a magic fix for common, yet easily managed, breastfeeding concerns I would have to say "yes, it is". The idea to pump instead of, or in conjunction with, breastfeeding is often suggested to mothers by their support people. These support people include other new mothers and experienced mothers at places like Mommy and Baby Yoga, Mommy and Me time, Kinder Music, Baby Signs, the museum, StarBucks, online support groups, mommy chats, any place mom's and babies hang out together; you all know where mommy's go. Other support people are their mothers and mother-in-laws, sisters, sisters-in-laws, aunts, grandma's, that old family friend; again, you know who these people are. Of course, other new mother's support people include Health Care Providers like doctors, nurses, midwives and the complementary support people like doula's and childbirth educators. And, in case you are not aware, these people include many that did not breastfeed themselves or were not successful in their attempts to breastfeed.
Most new moms have the intention of breastfeeding, as so as expected, it comes up in conversation. People feel the need to ask new moms how breastfeeding is going, new moms feel compelled to seek out support in these early weeks or health care providers are following up mom and baby. When moms are asked about breastfeeding they share the concerns they have with breastfeeding in hopes that someone can help them. Here is the list of common complaints and one likely answer they will receive to alleviate that concern. Sore Nipples -> Pump and bottle feed Baby not effectively sucking -> Pump and bottle feed Thrush -> Pump and bottle feed Engorged -> Pump between feeds Plugged Duct -> Pump between feeds or pump and bottle feed Needing to feed in public -> Pump and bottle feed Over Active Let Down -> Pump before feeding Low supply -> Pump between feeds or after feeds Baby not sleeping -> Pump and bottle feed or have someone else feed Colic -> Pump and have someone else feed Foremilk/Hindmilk concerns -> Pump before feeding It appears that pumping can be a common suggestion to alleviate the most probable breastfeeding issues. We need to be aware it is not a magic fix, it is most likely to be a band-aid, and it does not "fix" anything. We also need to be aware that pumping can create more issues. These are just a few ways this pumping band-aid could create more issues for mom and baby. With sore, bleeding, cracked nipples, generally the most common concern, generally easy to fix, pumping only results in double the work. Why would a new mother want to add in all the extra work of pumping and bottle feeding when getting some assistance with position and latch could make the problem go away, in even the very next feed? Or one of the many other solutions with have to help with the pain and healing. Often long term pumping is not going to sustain a babies needs and milk supply like breastfeeding directly from the breast would. Often breastfeeding relationships end far sooner than mother's intended due to supply issues because it leads to supplementation or another feeding method all together. This might not be the case all the time, as some mothers, do exclusively pump, but there is unique difference between a mother who makes the decision to exclusively pump compared to one who is trying to get baby nursing pain free at the breast and needing to pump in addition to. How about that baby that just is not sucking effectively or will not latch? Let's see, how do people learn? We learn by doing. If we take baby away from the breast, how does he learn? Again, we need to support moms and babies in positioning and latch and innate instincts that babies have to feed and let them learn together. If habitual placement is still not getting baby latching and sucking, we need to further evaluate what might be going on with that baby. Ignoring the difficulty baby is having and turning solely to the pump does not make the original issue baby was having go away. Thrush is no reason to stop feeding at the breast. The reality with pumping with thrush is that mothers now have more parts and equipment to treat or throw away. Thrush can sometimes take time to clear up but it spreads so easily, we need to restrict what comes into contact with the thrush to stop the spread of it, not add more to it. There are medication and alternatives that we can use to treat thrush and the discomfort of thrush as we are trying to eliminate the nasty little bug it is. Milk supply works on supply and demand so as well as pumping to relieve engorgement seems like a good idea right now, later on the fullness comes back and generally more full then the previous time, as a mother's body thinks that is milk that baby needed. If moms are engorged because a baby is not eating or draining the breast, then the answer is to get the baby eating and draining the breast, not pumping. The more baby is at the breast the less engorged mother's will be, assuming baby is eating well. Again, back up to latch and sucking. If baby is not waking to feed and mom is starting to fill up, mom can put baby to breast and encourage that baby to eat, to play his role in this breastfeeding relationship. Another concern with engorgement is that as much as it may seem logical that when mothers are engorged, it means they have a good, healthy milk supply, in fact the opposite can occur. The more often a women is engorged, the faster her milk supply will start to decreased. When breasts are full it sends a signal to the part of moms brain responsible for milk supply to slow production down and milk making cells start to shut down, resulting in less milk in the days ahead. Pumping when engorged can also pull more fluid, and not just milk, into the breast, resulting in edema. Often that fullness or edema is confused for milk and "good supply". Plugged ducts are uncomfortable, in fact down right painful, and yes moms want them out, but pumping is not the most effective way to unplug a plugged duct. In fact it can lead mom right back to the engorgement stage and create the spiral onwards from there, when the easiest way to get rid of that plug is by using baby, again, or some other strategies that are much more effective. I am starting to see a larger amount of women pumping so they can feed their baby while out and about. First, people that want to go out in public just need to accept that mothers and babies go out in public, too, and mothers and babies use breasts to feed. Secondly, mothers need to be informed about how this "solution" really is only one that is feasible for a small time. Each feed mom misses at the breast impacts that supply and demand mechanism again. If mom is out and is not feeding baby or replacing a feeding session without pumping again her body and brain communicate this to each other and the process of milk supply slows down. This again goes back to what I mention early about keeping up supply, supplementing and ending the relationship early than expected. Over Active Let Down is a problem that some moms struggle with but again pumping can just aggravate this problem. It is an easy problem to aggravate as it can lead to the engorgement issue and when baby is ready to feed, mom is ready to burst with milk and when the let down occurs it is like opening up a dam. Baby gets flooded with milk, has trouble managing flow, staying latched, becomes upset and this all causes frustration in mom and baby. Positioning, latch and frequent feeds are the easy fix here. On the other side of it, some babies have a hard time handling a normal let down, but it mimics and over-active let down. We need to be sure that we know if we have a baby that is struggling with a normal flow or a true over active let down. Another strategy I will mention here is block feeding. Block feeding used to be a common strategy for overactive let down but in more recent years, we have come to learn this is often detrimental to breastfeeding, as well. It appears to create a downward spiral of low intake, low weight gain and low milk supply. Always have what appears to be an overactive let down assessed by an IBCLC. For the healthy, full-term infant pumping for perceived low supply should be the last resort. Babies truly are the best solution here again; baby to breast = more milk in breast. Secondary low milk supply is a different issue and does not fall into the category of common yet easily managed breastfeeding concerns., which is what I am addressing here. I am also not addressing primary low milk supply which are maternal factors in less than 5% of mothers who do not make enough milk. These conditions should be determined with through evaluation with an IBCLC and primary health care providers. I am talking about common breastfeeding concerns that most mothers face. Pumping to top up or to force more milk into that non-sleeping baby:. Fuller tummy does not equal more sleep in babies. Babies have very small tummies, breastmilk is readily absorbed and digested so babies feed frequently. The issue here is not the amount of milk the baby takes, but rather unrealistic expectations and misunderstandings babies. If babies are really struggling with sleep, it is worthwhile seeking out a feeding assessment to ensure all the things above are not an issue. If baby is not gaining weight well and is also struggling with sleep, this is a different story. Colicky babies are much better soothed at the breast than any other way, pumping to feed another way removes that comfort source from this already high needs baby and can make the baby even more upset. There is no real understanding behind colic and why some babies are colicky and some are not but there is good understanding that skin-to-skin and mothering at the breast calms these babies best. Again, all things above should be ruled out before we just assume we have a colicky baby. I have also come to believe colic is an umbrella to other providers. I think sometimes we can seek some clarity on these babies and get past colic, rather than waiting it out. If you have what appears to be a colicky baby, perhaps booking for a breastfeeding session will give some of that clarity. Foremilk/hindmilk imbalance or what is being perceived as such seems to be rampant these days. It seems like a viral condition that has spread. So many moms seem to feel they have this issue, when in fact it is very rare. However, if a mother thinks this is an issue she has and pumps to get to the hindmilk, we go back to the engorgement cycle where mom has too much milk, can have a forceful let-down and then babies do get more foremilk than hindmilk, they are upset by the flow of milk and we end up in a vicious cycle. Worst case scenario, in fact, this could create that colicky baby we all fear. Foremilk/ hindmilk is best controlled by frequent feeds, proper positioning, good technique, etc. Mom's please seek out appropriate, knowledgeable, support when you encounter these easily managed breastfeeding concerns. So many families plan on breastfeeding before baby is even born. Initiation rates are 90%+ in hospitals but our stats show this drops off very quickly...less than 60% of mothers are meeting their own goals. A lot of people figure breastfeeding won't be too difficult or that they will just try and see how it goes. Many learn quickly that breastfeeding comes with lots of unexpected questions, confusion and lack of knowing what possible solutions are. When mothers find out they could have taken a class, they state how beneficial it would have been to receive some knowledge during pregnancy and know where to get guidance when they need it.  Taking a breastfeeding class with an International Board Certified Lactation Consultant (IBCLC) could help prevent many of the problems that mothers experience early on. A class will highlight common concerns and give you solutions to implement right away. You can also have the opportunity to ask questions that are individual to you. It also helps you establish a relationship with an IBCLC so you can feel more confident calling for help at the first signs of trouble. You will also learn about unique hospital policies and procedures. Taking a breastfeeding class should leave expecting parents feeling calm & confident about newborn baby behaviours and what to expect after baby is born and during their hospital stay. The topics covered in a breastfeeding class should include special circumstances, so if things with the birth do not go as expected, the parents are prepared with solutions, questions to ask their care providers and be informed about their options. They will also be informed about medical issues and an anatomical concerns that might have an impact on breastfeeding.
If there were previous breastfeeding problems in the past, it can be useful to take a class to help identify possible problem areas and make a plan of action for the next baby in case those issues (or others) come up again. I know so many times people say "why didn't anyone tell me". We are hear, ready to dish on it all! Really, are we ever prepared enough? Building your knowledge base and support team before you embark on your breastfeeding experience can make the whole thing a much different experience. I teach the majority of these classes at The Hive Wellness Studio. Topics always covered in the class are: Importance of breastfeeding Tips to successful breastfeeding How breastfeeding works Positions, breast crawl, attachment Hunger cues Intake, output Challenges & solutions and amore... Each registration include a breastfeeding booklet and is for one expecting parent and one support person. Register for a breastfeeding class now! When a woman plans to breastfeed her baby and that plan doesn't go accordingly, it can be a time of many emotions. This emotion is often referred to as "guilt". There is a common saying, "we shouldn't make women feel guilty for not being able to breastfeed." Of course, we shouldn't. There are so many factors, however it is not a black and white, can or can't, choose to or not, it works for some, not for others, etc. "Don't make her feel guilty" I don't want a mother to feel guilty, but I do want her to recognize her feelings about her situation. Feelings are not negative. Feelings are just feeling. And we need to feel to work through the struggles. We need to explore the feelings women experience when it comes to feeding their infant. Everything we see now is "Breast is Best". We have become a society that is "great" at encouraging breastfeeding but we are not a society that is even "good" at supporting and sustaining breastfeeding. This means many women are not meeting their breastfeeding goals. With that comes many feelings. Mothers who intended to breastfeed but struggle to meet that goal, feel a sense of loss. We know there is a connection to loss of breastfeeding and postpartum depression. We need to recognize that many mothers experience grief, and not guilt, in the postpartum period. I feel like grief is confused for guilt or a feeling of failure and it is not interchangeable. Mothers need to be given the opportunity to grieve what they had planned, what they believed postpartum would be like, the support they would receive but did not. Hearing “now, now dear, it’s ok, formula feeding is ok” doesn’t really help. It doesn’t help because it is not about breastmilk over formula. It’s about an expectation mothers had. It’s about a decision they thought they had control over, only to find out breastfeeding is difficult, but more so motherhood is difficult! It is all more difficult than society lets people believe. Breastfeeding is not well supported. It is not understood well. So many myths and wise tales still exist and are perpetuated daily, holding women back.  Women are finding themselves alone, feeling isolated & without reliable resources. Women who choose formula from the start don’t feel this way because they got to make that choice consciously. Women who planned to breastfeed but missed out on proper supports don’t feel like they had any other options but to give up their plans to breastfeed. That’s not a choice. That’s survival. We need to guide mothers to the appropriate, breastfeeding educated resources in a timely manner. Mothers deserve to have choices, someone who can offer solutions that are acceptable to them & who can provide support and counsel when breastfeeding isn't the best option for them.
Many mothers will be able to relate to this experience. The experience looks the same; a routine infant check up appointment, baby gets a weight check, the parents are asked some questions about development, etc. Upon looking at the weight, it is determined the infant is not gaining weight as expected. What does this mean? What is the cause? What should be done? It often is quite shocking to parents, especially mothers, to hear this news. They are perplexed because they thought feeding, usually breastfeeding, was going ok. How is it possible that baby isn’t gaining weight? How is it possible she didn’t know that baby wasn’t growing as expected? Can anything be done?  Common reasons provided for this phenomena is that mom has low milk supply, baby isn’t getting enough hind milk or baby is too sleepy and isn’t feeding often enough. I don’t think it is quite that simple.
What I find in these scenarios, because I get calls often after an experience like this, is that what is not communicated to the parents is why we do these checks, why they matter, what they mean and what should be done with the information. The simple answer is that we expect babes to maintain their own curve that they plotted on at birth (or more ideally 24 hours). When babies start to drop off that curve, this gives us a sign to look and assess what might be happening. This is a clue to ask some more questions and see if there are other pieces that can help tell us what might be happening. We want to know more about feeding behaviour, mood, output. Often what I hear is that there is no way baby needs to eat more. They are happy, content, sleep well, don’t really fuss. The opinion is that there is no way it is possible the baby isn't eating enough. People expect a hungry baby to cry, be irritable, to unsettled. I am going to say this is simply not true. I am sometimes more concerned about that “good baby” that sleeps well and always content. A very misunderstood piece of infant wellbeing is that weight gain influences appetite. What I mean by that, is that if a baby is gaining well, they demand to fed and show signs of being hungry regularly with easily identified feeding cues. What we think is a content baby because they have a calm mood, could be a baby who is content but not getting quite enough intake. A baby that is lower weight than expected, will have a lower appetite and will in fact cue less to be feed, will have subtle cues, likely won’t have a late hunger cueing & overall may make little fuss about it. If mother offers they will feed, but commonly have short feeding sessions. When they are being feed, their appetite is low so they do not do an efficient job, leading to milk being left in the breast and the body slowing down production. I give the example that if they are getting 70% of their intake requirement, they will eat at 70% efficiency (this will very baby to baby). This over time can cause a low supply, which influences their feeding because babies like flow...so low flow, means less interest in feeding and the cycle continues. If none of that concern is explained to a family, they leave these routine visits confused and bewildered as to why some one had a concern or what they could/should do about it and have no idea why it happened in the first place. There are lots of factors to consider to understand why this is happening & what the appropriate action for each case should be. If you are experiencing a difficult feeding situation where weight gain is a concern, booking a consult with an IBCLC is advisable. With a good assessment by an IBCLC, the root cause can often be determined and a solid plan can be put into place to get the baby fed, get weight gain concerns addressed, increase milk supply, maintain breastfeeding, etc. Other things to note in cases of lower than expected weight gain could be:
What is a Lactation Consultant, LC, IBCLC? The term lactation consultant or LC has become the known, accepted title for a professionals with expert knowledge in breastfeeding. They may work with moms and babies to address breastfeeding issues and concerns. They may also teach classes, assist with establishing breastfeeding one on one, and promote and protect breastfeeding through policy, procedure within health care and government. Origin of the term “Lactation Consultant The accepted term for “IBCLC” or International Board Certified Lactation Consultant in many geographical areas is "LC" or Lactation Consultant because, as you can see, that term is a mouthful. “LC” is not trademarked and does not hold the professional standard like “IBCLC” does, so one will occasionally find a practicing LC who is not an IBCLC. Consumers (mothers and families) and other professionals (doulas and doctors) need to be aware of this. As well, not all those who work as “lactation consultants” in health centres or breastfeeding support centres are IBCLCs. Some employers encourage employees to pursue the credential but don’t mandate it for employment. Many times, nurses with some basic breastfeeding education fill these jobs. Why is this IBC part so important? The International Board of Lactation Consultant Examiners (IBCLE) awards the title of International Board Certified Lactation Consultant to only the candidates who meet the comprehensive pathway requirements and pass an international exam. This allows IBLCE to establish the highest standards in lactation and breastfeeding care worldwide and to certify only the individuals who meet these standards. 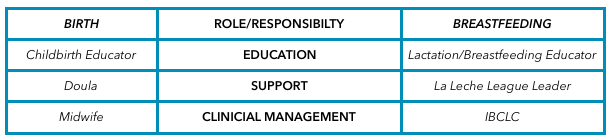 Breastfeeding education, support, clinical management Breastfeeding education, support, clinical management Breastfeeding alphabet soup I’d like to explain some of the breastfeeding alphabet soup by using the birthing support alphabet soup, as people seem to relate to that. All the roles are important, but they provide their own distinct scope, responsibilities, and abilities. They can all work together to provide comprehensive support. Primary roles of the individual bodies As you can see, I’ve broken this down into three primary roles. 1. Education 2. Support 3. Clinical management Education Educators teach you about the normal and expected processes of childbirth and breastfeeding. They typically call themselves childbirth educators and lactation educators. They teach the normal process of birth and what you can expect when having a baby, as well as encourage and promote breastfeeding. This information helps you make decisions, helps you know if you are on track, gives you references for getting the birth and breastfeeding relationships you want, and helps answer your questions. Educators typically teach community classes in group settings. Support Support people are typically those who have additional training in supporting mother, baby, and family during crucial times: birth and breastfeeding. They’re typically doulas and La Leche League (LLL) leaders. Doulas are usually paid professionals, and LLL is a mother-to-mother peer support group. These roles offer the encouragement and motivation you need to get through the processes of birth and breastfeeding. They are well versed in normal and expected outcomes. They know to watch for red flags to ensure they can guide you further if you have come outside the normal, expected process. Their job is to provide physical and emotional support, encouraging you to ask questions of your caregivers to make sure you’re well informed about what occurs. They have resources and guidelines to reassure you that you’re indeed in the realm of normal, and if things deviate from normal, they can point you in the direction of more resources. Clinical management Lastly, we have the clinical management professionals. These are the folks responsible for the clinical and medical bits of the scenario. They look at the facts and figures, big picture, and red flags to rule in or out the things that are not in the normal and expected category and then make management plans from there. They have the clinical experience of things that fall outside normal and how to manage them. Working together All of these people have a place in the realm of support and caregiving; what’s important is they know their role and responsibility and respect the others’. Where it becomes problematic is when the client receives something different from what she expected to receive. Sometimes, this occurs because the roles of each provider isn’t clear to her, and she might conclude that one person isn’t performing a role properly. Let’s look at how this might apply to IBCLCs specifically. In our example, a mother assumes that a breastfeeding educator* is an IBCLC. She notices that despite consulting with the helper, her breastfeeding issue remains unresolved. She decides to seek more help through a La Leche League leader, who determines that the issue is outside her scope and recommends an IBCLC. The mother insists that she already saw an IBCLC, but received no help. *this person could also be staff at a breastfeeding clinic or nurse who comes to her home This example is typical, and it hurts all support people. The educator gets a bad rep because she didn’t help. The LLL leader is helpless because the needs were outside her scope. The IBCLC profession gets a bad rep because the client misunderstood the different roles and expectations. Clients need to know clearly what their expectations are and who can best meet those expectations based on role, scope, and experience. I want to be asked and welcome being asked these questions! I want you to go and look at the IBLCE website to see what IBCLC's are all about and verify I am indeed and IBCLC and see what scope and standards are laid in place for my profession. I welcome the same questions about being a doula! I would love to see a blog about midwives and how they are different from doulas and childbirth educators (wink, wink, nudge, nudge midwives). All breastfeeding and lactation professionals have a responsibility to work together to ensure mothers have accurate information, so they can receive the support and encouragement they need as efficiently and as quickly as possible. Yes, I am a doula and many doulas offer placenta encapsulating as an additional service. I am not one of those doulas. I am a doula that is happy to refer that job out. Why? There are so many more evidence based things I can do to help new mothers that relate to most of the reasons why they are considering placenta encapsulating. There is simply not enough evidence for me to feel that this is how I would like to spend my time instead of doing the other things I can be doing for clients.  One of the primary reasons women consider encapsulating their placentas is anecdotal information that it can aid in appropriate milk supply. As an IBCLC, of course, I think milk supply is very significant. One of the driving factors of good production is good breastfeeding, early and often. This helps lay the foundation for the days and weeks to come. Breastfeeding, in fact, is one of the reasons I became a doula. We know that better birth experiences also aid in better breastfeeding. I wanted to support as many families as i could through the whole experience, rather than coming in after the birth and trying to catch up. Being there right away at birth and returning within 18-24 hours to see how things are progressing really helps get things off to a good start. Early identification of any potential roadblocks and removing them as soon as possible can make a big improvement to how breast-feeding starts off. There are so many reasons for milk supply being low. If as an IBCLC, we identify a supply issue and a suspect cause, knowing the mechanisms of some of the remedies available helps us know what to recommend to help resolve the issue. Ee do not yet know the mechanism of how placentas work to assist in lactation, if they even do. If we identify a supply risk, there are many more evidence based recommendations that can be made that we know with much more certainty should help the situation.
I will also state that I and other IBCLC colleagues have witnessed mothers with supply issues that resolve after they stop taking placenta capsules. Again, this speaks to us not knowing the mechanisms behind how a placenta might aid or impact lactation. In the end, my skill set as an IBCLC is of much more value than the time I would spend processing a placenta, in my opinion. I do also have some personal hesitations that I wish for people to consider. I am not saying that they need to decide not to encapsulate after the considerations but just that they consider the points. When we discuss postpartum mood imbalances & disorders we need to look at a larger picture than just a placenta. We see many mothers of multiples who state they did not consume their placenta after baby #1 but did after baby #2 and felt better emotionally than the first time. However, did they review the other differences? Baby #1 we often know little to nothing about what the experience of mothering will really be like, we go at it alone, we are not very confident in what we already know and we hesitate to seek out much information. Often baby #1 was a longer labour and longer pushing stage. Going from no baby to a baby, no sleep, constant physical and emotional demands from the infant, plus ones own recovery can be overwhelming. Baby #2, labour might be drastically different, maybe this time more supported, a shorter labour, easier pushing, the lack of sleep one gets with a newborn in the house is not as much as a surprise and there is much more understanding of normal newborn behaviours. Maybe the second time she had a doula, the same lady who encapsulated the placenta for her, and also provided postpartum supports, like helping with baby care so she could nap or helped with dishes and laundry so mom can rest, put up her feet and just focus on breastfeeding. Having some healthy meals with nutritional elements similar to a placenta might be a more regular occurrence the second time. Speaking of nutrients; sometimes it is said that mammals consume their own placentas, so why wouldn’t humans? Some theories are that mammals do it for safety; that in the wild the smell of afterbirth would draw predators near and the mother & the newly born were vulnerable and at risk, so for safety, the mother would quickly consume the placenta. There are also some theories that a mother would be hungry and in the wild food is scarce. Their own placenta vs nothing was the best they could get so it could be considered a last resort for a nutritional deficient animal. We no longer live in the wild and food scarcity is not as prevalent. In this day and age, most humans don’t look at their placenta and see their next meal or have a desire to consume it. Even in the wild, they consume it mostly in one sitting and not small amounts over days and weeks like the placenta encapsulation community recommends now. Even with diminished nutrition in food sources, we can purchase vitamins and foods enhanced with vitamins, which could provide the same effects. There is a study I am aware of that is not yet completed and it does show that the mothers consuming their placentas do have higher hemoglobins at 6 weeks postpartum. However, it has also been commented that there is a chance that the families that have the available monetary funds to pay for placenta encapsulation services, also have the monetary resources to purchases better quality and quantity of foods. The cost of the placenta encapsulations has not been covered for the study. It is a control that needs to be considered. As a former Medical Laboratory Technologist who worked in manufacturing of blood and blood products, I also worry about an appropriate environment to encapsulate and I do have concerns about infection control. I know that might be over-reactive but as someone who had to do quality control, sterility checks and saw the process of recalls, I think safety and specifications are important. I mean, after all, the placenta might be contaminated with poop. Even a small amount of bacteria can cause a big tummy ache. I say that more tongue in cheek than anything, but it is a thought. There is equipment needed to encapsulate and I am just not 100% that the risk of cross contamination is not there. Now, I am not an encapsulator and maybe there are steps in place to account for that risk. I am unsure about that. I am just saying, for me, it is something to think about. In the lab, in food processing, in other areas where contamination is a risk, sterility checks and quality control is what keeps stuff “clean and safe” and where recalls start, if they are needed. Just because you made the organ does not mean it cannot hurt you if bacteria is at play. After all that, we do know that placebo effect can be strong and powerful. I am happy to accept placebo effect if you are and I am happy to refer you to a local placenta encapsulator if your desire is to encapsulate your placenta.  Do you know what can mimic a tongue tie? Terrible breastfeeding technique can. The number one cause of many breastfeeding concerns or issues is positioning and latch. A good latch is vital to milk transfer. Good supply is dependent on milk transfer. Weight gain, pees and poops are dependent on supply. Swing back full circle to latch and latch is dependant on good positioning. This is true in the majority of cases. Add in that good positioning and latch should also make things easy, comfortable and pain free for mother. It should also make things easy, comfortable and effective for baby. When we see concerns with breastfeeding we must start with full maternal and infant assessment. This cannot be skipped. This includes a history on the birth and the start of breastfeeding, how feeding has been going, any know medical issues that contribute to breastfeeding concerns with mom and baby, a feeding assessment including positioning and latch, and structural exams of both mom and baby. Sometimes we have breastfeeding issues and concerns that are easy resolved by refining breastfeeding techniques. It can be that simple. Sometimes you will get breast-feeding technique (position and latch) perfect but there is still lots of trouble. We have pain, we have inadequate transfer, we have low weight, low pees and poops, etc. These are times we need to look further. There can be lots of reasons for this but today I am going to highlight tongue ties. Tongue tie or poor breastfeeding technique? I am all for fixing tongue ties. If they are a problem they are better resolved than to be “pushed on through”. However, I am more if favour of through assessment of breastfeeding & comprehensive follow up if a procedure is deemed warranted which is why I am drawing attention to this point today. Assessment of breastfeeding MUST include watching a feed amongst structurally examination of mothers and babies. And we have to address position and latch. The sooner we do this, the better. Why? Because if we have position and latch causing pain and damage, it is hard to tell if position changes are helping the pain or not. If we have damage and trauma, even a good latch will hurt until that is healed. So, then if look at a baby and see what visually looks like a tongue tie, we start to get blurred lines. The simple presence of a frenum is not a tongue tie. Diagnosing a tongue tie requires more than just looking. It is an assessment of function. Now when we are dealing with breastfeeding infants that function includes transfer of milk, weight gain, position needs, maternal comfort, visual of babies like folds in the lips, blanching of the frenum, blisters in the lips, etc. The people that can assist us in revision of ties are doctors and dentists and I am grateful to have them as part of our team. But, let me ask you how many doctors and dentists are watching feeds? How many would know how to throughly assess a breastfeeding session? How many know what to look for structurally in a mother? And throughly for an infant? Doctors and dentists that we rely on in resolution of breastfeeding concerns by revising tongue ties are typically only looking for a tongue tie as the reason to why you are presenting themselves to them. Their brains are actually wired to look for a possible intervention to try and resolve the issues based upon their skill level, experience and ability to help. Have you heard this quote before? “If you hear hooves behind you, don’t expect to see a zebra when you turn around. Chances are it’s a horse.” This means, first look for the simplest, common explanation to the problem presenting first. Once we have done this, then yes, we should go ahead and look for rarer & more problematic causes. In the medical community this is know as differential diagnosis. How do you know what is causing your breastfeeding issues? The most important key is to telling the difference between the horses and zebras. You cannot do this without a through evaluation, by a skilled practitioner. In the case of breastfeeding, these practitioners are International Board Certified Lactation Consultants. We have to be cautious of not assigning more importance to one element of breastfeeding than another, just because we think it is important or because we think the title of a certain practitioner is important or because that person thinks they are so important. There is another term for this which is “availability heuristic”. It is a bias towards things which you deem as more important because you readily recall it so deem it more probable. So, as someone looking at tongue ties most of the time this is front and centre in their minds. So, it is likely a dentist or doctor would go to tongue ties as a common cause of breastfeeding issues. As IBCLC’s we start at the basics, with the most common explanation of position and latch and move from there. The differential diagnosis mentioned about is what an IBCLC would do. This is why an IBCLC should be a first stop and why I think referrals for revisions of tongue ties should not be done without an IBCLC assessment. I bring this up because I am seeing moms & babies after tongue tie revisions who I didn’t see before. I don't know what the baby looked like before but more importantly what I am seeing a little more frequently than what I would like is bad breastfeeding technique. I cannot help but wonder, if we had just corrected positioning, would that have been enough. Did we have a true tie or did we have symptoms of bad technique that are also symptoms of tongue tie. Looking back at the information presented above about assessments, evaluations, horses and zebras & availability heuristic people you can see where my concern is warranted. Where do you go from here for support in resolving breastfeeding concerns? Be wise in your selection of care providers when you are struggling with breastfeeding. Step #1 should be an assessment with a skilled IBCLC. From there we will make all appropriate referrals to other members of our team that assist with getting breastfeeding back on track. If you are in Regina or in the Regina area, I would be happy to help you navigate your breast-feeding challenges. You can give me a call or easily book online.  Nipples sore?
Sore nipples can be one of the more common breast-feeding challenges. You certainly are not alone in this, however, you don't need to remain sore, or worse yet, in pain. Pain at any point is your bodies way of telling you something is wrong and you need to pay attention to yourself. What causes soreness and pain? Most commonly it is because of trouble with positioning and latch, creating friction, and proceeding them to soreness, cracks, blisters, bleeding and sometimes infections and even lose of skin. What can be done? Here are a few quick ideas. Most importantly, check your position and your comfort. One of my rules is to make sure mom is comfortable first. Ideally, mothers are slightly reclined, arms and shoulders lose and down, and her neck has the ability to be relaxed. With this, mothers can then bring baby to them. You don't want to try to take your breast to baby. Baby can be front-to-front with mom, being supported by mother’s arms, and mother’s arms can be supported with pillows. Use gravity to help baby get on the breast deeper, rather than sitting upright and having gravity pull baby down or away from the breast. If we still have discomfort, we need to check baby’s latch. A good latch is vital to comfort but also to long term duration of breastfeeding. A good latch is key to effective feeding which is essential for adequate milk supply. You might need to ask someone for help with checking the latch. If someone tells you it looks good, but you have pain during or after a feed, you need to ask someone else. If position changes do not help with latching issues and soreness and pain are still prevailing sometimes we need to look farther into reasons and makes plans. Sometimes we can use a nipple shield to help protect the nipple and help baby to latch. It is important to get good help if needing a shield. There are important things to watch for such as fitting, proper placement, adequate milk transfer, babies output and weight gain. This is very important to know and recognize however; nipple shields are a Band-aid solution. They are not an answer, they are simply a tool to help keep the baby breastfeeding, at the breast, rather than quitting breast-feeding or going to pumping and feeding another way. It is a short term tool that needs a bigger plan. Throw away the lanolin! For years we were told Lanolin was fabulous and all new mothers needed it. But the new research shows us, doing nothing is actually more effective than lanolin and in fact lanolin can delay healing, making things even worse for a longer period of time. Mor effectively you can apply breastmilk to the nipple or coconut oil or calendula if you want to try something else. Do not let you nipples be wet and cold at the same time. Again, we were told for years that we should let the nipples air dry. But for mother’s with very sore, damaged nipples, the cool air can cause more harm. It is a good idea to apply heat while the nipple dries. Something like a rice sock or heating pad after baby unlatches, or even when getting out of the shower or bath, can help. This helps bring blood flow to the nipple that previously was restricted. Soreness and pain are not considered normal for breastfeeding at any time or for any length of time. If basic positioning and latch changes do not help, it is worth having someone skilled come and have a look. They can help assess and evaluate what might be happening and help you make a plan to further overcome the struggles.  What do we really know about breastfeeding? Really? We are 3 generations into formula feeding. It’s been said it takes 100 years to make change and make things the norm. Well, indeed, this has worked for formula feeding. That is by far the most common method of feeding infants DESPITE a whopping 90+% initiation rate in our country. We are failing more than we are succeeding which tells me we don't really get it. Why are we so quick to start supplementing or letting go of breastfeeding? What steps are we walking before we made that decision, if any? We should be working to remedy breastfeeding but this idea that we can supplement while we remedy breastfeeding, isn't a wise one. I am not saying supplements are not needed at times but I am saying that our helpers should know how to work with breastfeeding first and foremost.
Why are only a quarter of babies getting any breastmilk by the middle of their first year? A very large part of it is that there is a fabulous amount of interference. Interference comes from all over and starts long before babies are even born. Dare I say this interference starts before most babies are even conceived? Let’s look at media. Let’s look at the propaganda all over medical establishments, directed both at patients and at medical professionals. Let’s look at our own communities and then our own families. What is the message out there reaching people? Could this be part of why we are not able to help remedy breastfeeding? They are certainly not breastfeeding friendly messages. But, let’s say you get through all of that and to the people that are supposed to be promoting and supporting breastfeeding. You know what? You still will here a large amount of variants in what these people say and recommend you do. From basics of position and latch to troubleshooting concerns, it seems very few of us on are the same page. It is highly frustrating as a professional and I know it is highly frustrating as a parent. It honestly makes me ask myself, what do we know about breastfeeding? For many years I was involved with a peer support group. Within this group I was told that this is where we see normal breastfeeding. It was a well-established group with many, many years of experience in breastfeeding. This was my introduction to breastfeeding outside my own experience and being able to view and witness many dyads and what breastfeeding looked like for others. It was amazing and eye-opening. I learnt lots and went on to learn more and become a peer-volunteer to help mothers that were struggling. I was all in. Consuming all I could to try and figure out the barriers to successful breast-feeding. I had a big blue book full of breastfeeding information. I studied it. I did activities and exercises to help me expand topics. I read and read and discussed breastfeeding at great length. I was accredited and able to start helping moms. Moms would call me with concerns and I would look up moms concerns and then read to them from the book what the strategies were to help them overcome their challenges. I very often never heard back from these mothers to know if things resolved or not. I am hopeful many mothers did better and were successful but I know now that lots did not. I saw many moms in person return to meetings month after month and got to know many of these dyads well. We told mothers what they could do right to make breastfeeding work well and especially how if people didn’t interfere all would be good for them. Feed early and often and supply would be there. Don't have pain meds in labour and baby will breastfeed well. Stay away from bottles & supplements and pacifiers and just feed and feed and feed. Yet, that didn’t work for everyone. I really was perplexed as to why. After a few years of this, that is when I decided to expand my education and knowledge and scope of practice. I was going to pursue being an IBCLC. I mean, I knew normal breastfeeding, right? How hard could it be? Was becoming an IBCLC easy? Not at all. Was it hard? Yes, indeed. On so many levels. I was shocked when I started getting assignments back with really low grades. So many wrong answers. But how? I KNOW breastfeeding. I have been helping moms for years. I have these answers in a big blue book. It says here in black and white this is how breastfeeding works and this is what you do to overcome the struggles. It was wrong? How could it be wrong? How many women did I tell this info to? And how many of my friends did what the book said. This is how breastfeeding is, this is the normal for breastfeeding and all moms and babies are different and that’s ok. But I came to learn, yes, some concerns are common but there are actually tighter perimeters on what is “normal” and expected. I was pointed in a new direction for learning. My beliefs shifted in a few ares. Change is hard. But I was changed. I started seeing stuff in different ways, through many different eyes, many different versions and was taking a critical look at what I knew and what I was learning and the work of many others. I learnt about growth charts and poop (oh how I love to talk poop now), infant sleep, tummy time, newborn weight gain and loss, milk supply, medications, medical conditions, how to supplement and when it actually is helpful, and how much happier and less stressed some moms and babies (and their families) could be and how to screen the bigger picture. I learnt more than how to tell moms more than “this too shall pass” & “some babies are just like that”. I also learnt that professionals don't agree on a large number of topics. Weight loss, sleep, pain, creams, positioning. When and why did someone decide that 7% loss if ok, but 10% means we must supplement? Why do some think there should be zero weight loss at birth and some think it is acceptable to take 2 or 3 weeks to get back to birth weight? Why do big babies need to be supplemented an hour after birth but small babies are ok? Why do some say that sore nipples is a right of passage and some think there should be no pain, ever? Why are some nursing babies like footballs and other think we rarely should do this? This list could go on and on. For some of use we come to our own conclusions based on clinical experience and patterns and outcomes that we see. Some of us just read the guidelines laid out for us because that is how it has always been done. Some of us are halfway between. Some of us come from a place of our own experiences and judgement and biases that come from that. (The latter is really not best practice and we need to learn how to detach from our own experiences to look at the current evidence in front of us.) Some of started in one place and have landed in another. I can say that I believe I do have good evidence based research to back my opinions on many of those questions, plus many others. I have protocols and practices that I use over and over with success with families, but am happy to say as much as they are protocols they are very flexible and can be defined differently for each family. I haven't stopped seeing stuff in different ways, through many different eyes, many different versions and haven't stopped taking a critical look what is happening with my clients and figuring out how I can best help them met their goals. Ladies (& partners and support people), you need to know that there are resources out there to help you, when you need it, where you need it and that will consider YOUR goals. I can come to your home, I can come to see you at the hospital, you can come to my office. If you feel like you are not getting the support you need, when you need it, don't throw in the towel on breastfeeding. There are always options. Breastfeeding can take some time to get established. It is a learned behaviour by both mother and baby, and each baby a woman has is a new learning experience. With that said, time is also precious when trying to get breastfeeding established. Some things are normal learning curve experiences and some things are not normal and should be addressed as soon as possible. Mother's almost always know when something is not correct. I spoke with a mother earlier this week who knew something wasn't right. She asked for a referral to a lactation consultant and was denied. She continued to ask as the days went on and was told repeatedly that what she was experiencing was normal and wasn't yet at the point of needing a lactation consultant. Her frustration was to the point that she was ready to throw in the towel on breastfeeding. She spoke to a friend who informed her that there are private IBCLC's who she could see and who would be able to see her sooner than later and that before she quit breastfeeding she should call me. This mother took the advice of the friend and gave me a call. I was able to listen to her breastfeeding story to date, do an assessment on her and baby, figure out what her goals for breastfeeding were and prioritize the concerns she had about breastfeeding. Sometimes it is about addressing one big issue, like the amount of pain a mother is having, and then moving forward with other plans and goals. Breaking it down into manageable bits and pieces can make the big picture seem far less daunting. Let's not worry about breastfeeding until baby is one year, if we are not even sure we are going to make one week with the amount of pain we have. Maybe we should look at how to get rid of the pain, and see how week two goes…sounds far less scary than pain for a year.
 white color that can often been seen after feedings white color that can often been seen after feedings You are a new breastfeeding mother. It has been about ten days and your cracked bleeding nipples aren't healing & you have started to have a burning sensation with deep throbbing pain in your breast. It sometimes lasts for a few minutes, but sometimes hours. The beginning of feeds are terrible and even between feeds you are getting electrical shock like feelings in the breast. If this is you, you are like many other mothers and like many other mothers you may have been told you have thrush. You are given a prescription for nystatin for you and baby. You treat for two weeks and symptoms get mildly better, but it isn't going away. Baby has no symptoms but your pain just won't knock it off. You get Nystatin for a couple more weeks, cut out all sugars, start washing your nipples with grape seed extract and the pain in still persistent. Maybe you have had APNO cream & some Diflucan in there, as well. Still no success.
How about I suggest to you that if you have thrown every thrush treatment at your nipples and you're not seeing results, that it isn't really thrush you are trying to treat? Thrush is very commonly diagnosed, rather misdiagnosed. I do not think that it is as common as we are being led to believe it is. I know you are asking me, "if it isn't thrush than what is it?" I would say in more likelihood than not, it is vasospasms. Vado-Whats? What are those? The simple answer is that the blood vessels in the are contracting and becoming smaller in diameter - called vasospasms. This can happen for a variety of reason and for some people it can be very painful and occur in various parts of the body, including the nipple in breastfeeding mothers. There are risk factors for vasospasms including but not limited to :
What are some more symptoms and how would you suspect you have vasospasms?
It is important to seek professional help as soon as possible if this problem is persistent. They can help assess the cause and come up with some remedies for you. They can also explain the use of vitamins, minerals and omega fatty acids (important for healing). There are also prescription medications available, if warranted, and your IBCLC and physician can help accommodate that. You do not need to suffer through the pain or end breastfeeding for this to resolve. If you would like to keep breastfeeding, without pain, book an appointment and we can get you back on track. |
Kim Smith
|
 RSS Feed
RSS Feed

|
|
Quick facts:
International Board Certified Lactation Consultant (2010), Re-certified (2015, 2020) TummyTime Method Instructor Retired Doula, CAPPA trained, Pre-Certified ProDoula (2009) Your Birth Experience (YBE) Certified (2015) Wife & mother of 4 Retired Medical Laboratory Technologist |