|
I get asked about infants stooling patterns quite a lot, typically from worried mothers who have an infant who has slowed down on stooling, maybe 1-2 days, sometimes 7-10 days. The baby might also be gassy, not sleeping or fussy. Moms often will ask various sources if this is normal or expected. I was certainly taught to believe this with a variety of reasons as to why. As an IBCLC I don’t consider this to be normal, anymore, and I will list some of the reasons as to why later. In my opinion, the information I had been provided over a decade ago is still how health professionals and peer support are being taught in their education and orientation to units and job positions that support infants and mothers is also teaching this way. The number one reason I hear is that breastmilk is just highly digestible & there is nothing left to dispose of. My common sense response to those who say ‘it’s just absorbed’, is why then when babies finally do have a bowel movement is it always reported as “a huge blow out” or why do babies have “poop days”. The days are described as days where, once the stooling starts, it does not stop for several diaper hours. If it was readily absorbed, it wouldn’t be an explosion or take hours to clear out the bowels. In recent years more information has come out to tell us that, in fact, there are known constituents in breastmilk that are not digestible. One specific component is human milk sugars that are attached to the lactose molecule in breastmilk. They can make up to 20% of the content of milk. So, to think that ⅕ of the intake of what an infant consumes is not digestible, makes one wonder where it goes. It appears though, that this doesn’t have a role in nutrition, but instead in gut health. The bacteria of the infant gut is what thrives on these human milk sugars, not so much that an infant's growth thrives here. This could be one of the reasons why we may often see a baby gaining weight well, but not be stooling. But we might see a colicy or gassy baby, because the gut flora isn’t quite ideal. I find often getting more milk into the baby helps these symptoms. More milk = more human milk sugars = more healthy bacteria. Not to mention other little things that end up in stool. The process of digestion alone would have some sort of byproduct left, even just the epithelial cells of the digestive tract sloughing off along the way.  Baby not pooping? 3 days? 10 days? Is this normal? I stated the number one reason that I hear as a reason why babies might not be stooling is that people believe breastmilk is digestible and I have provided some reasons as to why this is not true. But, I am actually more concerned about another aspect of the non-stooling situation, beyond just human milk sugars and bacteria content. I have shown my belief of *if milk is going in, stools need to be coming out”. When I come across a non-stooling infant, I want to have a look at the growth patterns of these infants. I mentioned thriving infants above because it is very important to discuss infant weight gain in all of this. Watching just pee alone is dangerous as babies can get to a pretty scary place before they start to really slow down on the peeing and may be in a state of failure-to-thrive at that point. We can possibly avoid that by watching stooling. I will say it one of the first signs of lower than required intake in many many babies I have worked with. This can all actually have a long term effect on breastfeeding. As babies take in less milk & have slow or no weight gain , milk supply can be lowered, resulting in even less milk being taken in by the baby and the cycle continues. It can also be a sign of more going on and the sooner we intervene and assess the situation, the sooner we can strategize solutions to prevent things from a downward spiral. What should we expect in a babies diaper then? This is what I recommend. As babies get closer to 4 months, they may slow down to 2-3 diapers a day, but in the early days and weeks fore sure with each good feed or couple feeds, there should be a bowel movement. 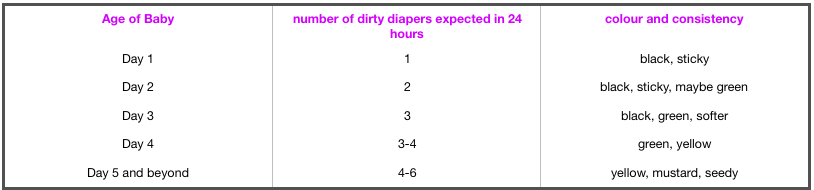 I also want to mention that these ideas and supporting information is quite new, so just like we have to be patient with babies and how they grow and change and develop, we have to be patient with the research and learning of the changes and developments coming out in breastfeeding. As much as we have been breastfeeding “forever”, it was a time before so much evidence and research existed and was desired.
If you are concerned about your babies stooling patterns, I am always happy to help explore that with you. I welcome you to reach out for a consult, in person or virtually. (originally posted Feb 21...I am sure more will be added as time and linked thoughts come up)  If I asked myself if pumping was being used as a magic fix for common, yet easily managed, breastfeeding concerns I would have to say "yes, it is". The idea to pump instead of, or in conjunction with, breastfeeding is often suggested to mothers by their support people. These support people include other new mothers and experienced mothers at places like Mommy and Baby Yoga, Mommy and Me time, Kinder Music, Baby Signs, the museum, StarBucks, online support groups, mommy chats, any place mom's and babies hang out together; you all know where mommy's go. Other support people are their mothers and mother-in-laws, sisters, sisters-in-laws, aunts, grandma's, that old family friend; again, you know who these people are. Of course, other new mother's support people include Health Care Providers like doctors, nurses, midwives and the complementary support people like doula's and childbirth educators. And, in case you are not aware, these people include many that did not breastfeed themselves or were not successful in their attempts to breastfeed.
Most new moms have the intention of breastfeeding, as so as expected, it comes up in conversation. People feel the need to ask new moms how breastfeeding is going, new moms feel compelled to seek out support in these early weeks or health care providers are following up mom and baby. When moms are asked about breastfeeding they share the concerns they have with breastfeeding in hopes that someone can help them. Here is the list of common complaints and one likely answer they will receive to alleviate that concern. Sore Nipples -> Pump and bottle feed Baby not effectively sucking -> Pump and bottle feed Thrush -> Pump and bottle feed Engorged -> Pump between feeds Plugged Duct -> Pump between feeds or pump and bottle feed Needing to feed in public -> Pump and bottle feed Over Active Let Down -> Pump before feeding Low supply -> Pump between feeds or after feeds Baby not sleeping -> Pump and bottle feed or have someone else feed Colic -> Pump and have someone else feed Foremilk/Hindmilk concerns -> Pump before feeding It appears that pumping can be a common suggestion to alleviate the most probable breastfeeding issues. We need to be aware it is not a magic fix, it is most likely to be a band-aid, and it does not "fix" anything. We also need to be aware that pumping can create more issues. These are just a few ways this pumping band-aid could create more issues for mom and baby. With sore, bleeding, cracked nipples, generally the most common concern, generally easy to fix, pumping only results in double the work. Why would a new mother want to add in all the extra work of pumping and bottle feeding when getting some assistance with position and latch could make the problem go away, in even the very next feed? Or one of the many other solutions with have to help with the pain and healing. Often long term pumping is not going to sustain a babies needs and milk supply like breastfeeding directly from the breast would. Often breastfeeding relationships end far sooner than mother's intended due to supply issues because it leads to supplementation or another feeding method all together. This might not be the case all the time, as some mothers, do exclusively pump, but there is unique difference between a mother who makes the decision to exclusively pump compared to one who is trying to get baby nursing pain free at the breast and needing to pump in addition to. How about that baby that just is not sucking effectively or will not latch? Let's see, how do people learn? We learn by doing. If we take baby away from the breast, how does he learn? Again, we need to support moms and babies in positioning and latch and innate instincts that babies have to feed and let them learn together. If habitual placement is still not getting baby latching and sucking, we need to further evaluate what might be going on with that baby. Ignoring the difficulty baby is having and turning solely to the pump does not make the original issue baby was having go away. Thrush is no reason to stop feeding at the breast. The reality with pumping with thrush is that mothers now have more parts and equipment to treat or throw away. Thrush can sometimes take time to clear up but it spreads so easily, we need to restrict what comes into contact with the thrush to stop the spread of it, not add more to it. There are medication and alternatives that we can use to treat thrush and the discomfort of thrush as we are trying to eliminate the nasty little bug it is. Milk supply works on supply and demand so as well as pumping to relieve engorgement seems like a good idea right now, later on the fullness comes back and generally more full then the previous time, as a mother's body thinks that is milk that baby needed. If moms are engorged because a baby is not eating or draining the breast, then the answer is to get the baby eating and draining the breast, not pumping. The more baby is at the breast the less engorged mother's will be, assuming baby is eating well. Again, back up to latch and sucking. If baby is not waking to feed and mom is starting to fill up, mom can put baby to breast and encourage that baby to eat, to play his role in this breastfeeding relationship. Another concern with engorgement is that as much as it may seem logical that when mothers are engorged, it means they have a good, healthy milk supply, in fact the opposite can occur. The more often a women is engorged, the faster her milk supply will start to decreased. When breasts are full it sends a signal to the part of moms brain responsible for milk supply to slow production down and milk making cells start to shut down, resulting in less milk in the days ahead. Pumping when engorged can also pull more fluid, and not just milk, into the breast, resulting in edema. Often that fullness or edema is confused for milk and "good supply". Plugged ducts are uncomfortable, in fact down right painful, and yes moms want them out, but pumping is not the most effective way to unplug a plugged duct. In fact it can lead mom right back to the engorgement stage and create the spiral onwards from there, when the easiest way to get rid of that plug is by using baby, again, or some other strategies that are much more effective. I am starting to see a larger amount of women pumping so they can feed their baby while out and about. First, people that want to go out in public just need to accept that mothers and babies go out in public, too, and mothers and babies use breasts to feed. Secondly, mothers need to be informed about how this "solution" really is only one that is feasible for a small time. Each feed mom misses at the breast impacts that supply and demand mechanism again. If mom is out and is not feeding baby or replacing a feeding session without pumping again her body and brain communicate this to each other and the process of milk supply slows down. This again goes back to what I mention early about keeping up supply, supplementing and ending the relationship early than expected. Over Active Let Down is a problem that some moms struggle with but again pumping can just aggravate this problem. It is an easy problem to aggravate as it can lead to the engorgement issue and when baby is ready to feed, mom is ready to burst with milk and when the let down occurs it is like opening up a dam. Baby gets flooded with milk, has trouble managing flow, staying latched, becomes upset and this all causes frustration in mom and baby. Positioning, latch and frequent feeds are the easy fix here. On the other side of it, some babies have a hard time handling a normal let down, but it mimics and over-active let down. We need to be sure that we know if we have a baby that is struggling with a normal flow or a true over active let down. Another strategy I will mention here is block feeding. Block feeding used to be a common strategy for overactive let down but in more recent years, we have come to learn this is often detrimental to breastfeeding, as well. It appears to create a downward spiral of low intake, low weight gain and low milk supply. Always have what appears to be an overactive let down assessed by an IBCLC. For the healthy, full-term infant pumping for perceived low supply should be the last resort. Babies truly are the best solution here again; baby to breast = more milk in breast. Secondary low milk supply is a different issue and does not fall into the category of common yet easily managed breastfeeding concerns., which is what I am addressing here. I am also not addressing primary low milk supply which are maternal factors in less than 5% of mothers who do not make enough milk. These conditions should be determined with through evaluation with an IBCLC and primary health care providers. I am talking about common breastfeeding concerns that most mothers face. Pumping to top up or to force more milk into that non-sleeping baby:. Fuller tummy does not equal more sleep in babies. Babies have very small tummies, breastmilk is readily absorbed and digested so babies feed frequently. The issue here is not the amount of milk the baby takes, but rather unrealistic expectations and misunderstandings babies. If babies are really struggling with sleep, it is worthwhile seeking out a feeding assessment to ensure all the things above are not an issue. If baby is not gaining weight well and is also struggling with sleep, this is a different story. Colicky babies are much better soothed at the breast than any other way, pumping to feed another way removes that comfort source from this already high needs baby and can make the baby even more upset. There is no real understanding behind colic and why some babies are colicky and some are not but there is good understanding that skin-to-skin and mothering at the breast calms these babies best. Again, all things above should be ruled out before we just assume we have a colicky baby. I have also come to believe colic is an umbrella to other providers. I think sometimes we can seek some clarity on these babies and get past colic, rather than waiting it out. If you have what appears to be a colicky baby, perhaps booking for a breastfeeding session will give some of that clarity. Foremilk/hindmilk imbalance or what is being perceived as such seems to be rampant these days. It seems like a viral condition that has spread. So many moms seem to feel they have this issue, when in fact it is very rare. However, if a mother thinks this is an issue she has and pumps to get to the hindmilk, we go back to the engorgement cycle where mom has too much milk, can have a forceful let-down and then babies do get more foremilk than hindmilk, they are upset by the flow of milk and we end up in a vicious cycle. Worst case scenario, in fact, this could create that colicky baby we all fear. Foremilk/ hindmilk is best controlled by frequent feeds, proper positioning, good technique, etc. Mom's please seek out appropriate, knowledgeable, support when you encounter these easily managed breastfeeding concerns. When a woman plans to breastfeed her baby and that plan doesn't go accordingly, it can be a time of many emotions. This emotion is often referred to as "guilt". There is a common saying, "we shouldn't make women feel guilty for not being able to breastfeed." Of course, we shouldn't. There are so many factors, however it is not a black and white, can or can't, choose to or not, it works for some, not for others, etc. "Don't make her feel guilty" I don't want a mother to feel guilty, but I do want her to recognize her feelings about her situation. Feelings are not negative. Feelings are just feeling. And we need to feel to work through the struggles. We need to explore the feelings women experience when it comes to feeding their infant. Everything we see now is "Breast is Best". We have become a society that is "great" at encouraging breastfeeding but we are not a society that is even "good" at supporting and sustaining breastfeeding. This means many women are not meeting their breastfeeding goals. With that comes many feelings. Mothers who intended to breastfeed but struggle to meet that goal, feel a sense of loss. We know there is a connection to loss of breastfeeding and postpartum depression. We need to recognize that many mothers experience grief, and not guilt, in the postpartum period. I feel like grief is confused for guilt or a feeling of failure and it is not interchangeable. Mothers need to be given the opportunity to grieve what they had planned, what they believed postpartum would be like, the support they would receive but did not. Hearing “now, now dear, it’s ok, formula feeding is ok” doesn’t really help. It doesn’t help because it is not about breastmilk over formula. It’s about an expectation mothers had. It’s about a decision they thought they had control over, only to find out breastfeeding is difficult, but more so motherhood is difficult! It is all more difficult than society lets people believe. Breastfeeding is not well supported. It is not understood well. So many myths and wise tales still exist and are perpetuated daily, holding women back.  Women are finding themselves alone, feeling isolated & without reliable resources. Women who choose formula from the start don’t feel this way because they got to make that choice consciously. Women who planned to breastfeed but missed out on proper supports don’t feel like they had any other options but to give up their plans to breastfeed. That’s not a choice. That’s survival. We need to guide mothers to the appropriate, breastfeeding educated resources in a timely manner. Mothers deserve to have choices, someone who can offer solutions that are acceptable to them & who can provide support and counsel when breastfeeding isn't the best option for them.
What is a Lactation Consultant, LC, IBCLC? The term lactation consultant or LC has become the known, accepted title for a professionals with expert knowledge in breastfeeding. They may work with moms and babies to address breastfeeding issues and concerns. They may also teach classes, assist with establishing breastfeeding one on one, and promote and protect breastfeeding through policy, procedure within health care and government. Origin of the term “Lactation Consultant The accepted term for “IBCLC” or International Board Certified Lactation Consultant in many geographical areas is "LC" or Lactation Consultant because, as you can see, that term is a mouthful. “LC” is not trademarked and does not hold the professional standard like “IBCLC” does, so one will occasionally find a practicing LC who is not an IBCLC. Consumers (mothers and families) and other professionals (doulas and doctors) need to be aware of this. As well, not all those who work as “lactation consultants” in health centres or breastfeeding support centres are IBCLCs. Some employers encourage employees to pursue the credential but don’t mandate it for employment. Many times, nurses with some basic breastfeeding education fill these jobs. Why is this IBC part so important? The International Board of Lactation Consultant Examiners (IBCLE) awards the title of International Board Certified Lactation Consultant to only the candidates who meet the comprehensive pathway requirements and pass an international exam. This allows IBLCE to establish the highest standards in lactation and breastfeeding care worldwide and to certify only the individuals who meet these standards. 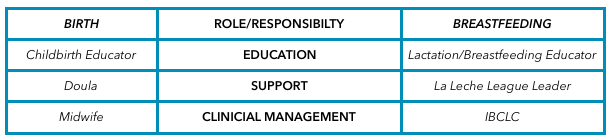 Breastfeeding education, support, clinical management Breastfeeding education, support, clinical management Breastfeeding alphabet soup I’d like to explain some of the breastfeeding alphabet soup by using the birthing support alphabet soup, as people seem to relate to that. All the roles are important, but they provide their own distinct scope, responsibilities, and abilities. They can all work together to provide comprehensive support. Primary roles of the individual bodies As you can see, I’ve broken this down into three primary roles. 1. Education 2. Support 3. Clinical management Education Educators teach you about the normal and expected processes of childbirth and breastfeeding. They typically call themselves childbirth educators and lactation educators. They teach the normal process of birth and what you can expect when having a baby, as well as encourage and promote breastfeeding. This information helps you make decisions, helps you know if you are on track, gives you references for getting the birth and breastfeeding relationships you want, and helps answer your questions. Educators typically teach community classes in group settings. Support Support people are typically those who have additional training in supporting mother, baby, and family during crucial times: birth and breastfeeding. They’re typically doulas and La Leche League (LLL) leaders. Doulas are usually paid professionals, and LLL is a mother-to-mother peer support group. These roles offer the encouragement and motivation you need to get through the processes of birth and breastfeeding. They are well versed in normal and expected outcomes. They know to watch for red flags to ensure they can guide you further if you have come outside the normal, expected process. Their job is to provide physical and emotional support, encouraging you to ask questions of your caregivers to make sure you’re well informed about what occurs. They have resources and guidelines to reassure you that you’re indeed in the realm of normal, and if things deviate from normal, they can point you in the direction of more resources. Clinical management Lastly, we have the clinical management professionals. These are the folks responsible for the clinical and medical bits of the scenario. They look at the facts and figures, big picture, and red flags to rule in or out the things that are not in the normal and expected category and then make management plans from there. They have the clinical experience of things that fall outside normal and how to manage them. Working together All of these people have a place in the realm of support and caregiving; what’s important is they know their role and responsibility and respect the others’. Where it becomes problematic is when the client receives something different from what she expected to receive. Sometimes, this occurs because the roles of each provider isn’t clear to her, and she might conclude that one person isn’t performing a role properly. Let’s look at how this might apply to IBCLCs specifically. In our example, a mother assumes that a breastfeeding educator* is an IBCLC. She notices that despite consulting with the helper, her breastfeeding issue remains unresolved. She decides to seek more help through a La Leche League leader, who determines that the issue is outside her scope and recommends an IBCLC. The mother insists that she already saw an IBCLC, but received no help. *this person could also be staff at a breastfeeding clinic or nurse who comes to her home This example is typical, and it hurts all support people. The educator gets a bad rep because she didn’t help. The LLL leader is helpless because the needs were outside her scope. The IBCLC profession gets a bad rep because the client misunderstood the different roles and expectations. Clients need to know clearly what their expectations are and who can best meet those expectations based on role, scope, and experience. I want to be asked and welcome being asked these questions! I want you to go and look at the IBLCE website to see what IBCLC's are all about and verify I am indeed and IBCLC and see what scope and standards are laid in place for my profession. I welcome the same questions about being a doula! I would love to see a blog about midwives and how they are different from doulas and childbirth educators (wink, wink, nudge, nudge midwives). All breastfeeding and lactation professionals have a responsibility to work together to ensure mothers have accurate information, so they can receive the support and encouragement they need as efficiently and as quickly as possible. Yes, I am a doula and many doulas offer placenta encapsulating as an additional service. I am not one of those doulas. I am a doula that is happy to refer that job out. Why? There are so many more evidence based things I can do to help new mothers that relate to most of the reasons why they are considering placenta encapsulating. There is simply not enough evidence for me to feel that this is how I would like to spend my time instead of doing the other things I can be doing for clients.  One of the primary reasons women consider encapsulating their placentas is anecdotal information that it can aid in appropriate milk supply. As an IBCLC, of course, I think milk supply is very significant. One of the driving factors of good production is good breastfeeding, early and often. This helps lay the foundation for the days and weeks to come. Breastfeeding, in fact, is one of the reasons I became a doula. We know that better birth experiences also aid in better breastfeeding. I wanted to support as many families as i could through the whole experience, rather than coming in after the birth and trying to catch up. Being there right away at birth and returning within 18-24 hours to see how things are progressing really helps get things off to a good start. Early identification of any potential roadblocks and removing them as soon as possible can make a big improvement to how breast-feeding starts off. There are so many reasons for milk supply being low. If as an IBCLC, we identify a supply issue and a suspect cause, knowing the mechanisms of some of the remedies available helps us know what to recommend to help resolve the issue. Ee do not yet know the mechanism of how placentas work to assist in lactation, if they even do. If we identify a supply risk, there are many more evidence based recommendations that can be made that we know with much more certainty should help the situation.
I will also state that I and other IBCLC colleagues have witnessed mothers with supply issues that resolve after they stop taking placenta capsules. Again, this speaks to us not knowing the mechanisms behind how a placenta might aid or impact lactation. In the end, my skill set as an IBCLC is of much more value than the time I would spend processing a placenta, in my opinion. I do also have some personal hesitations that I wish for people to consider. I am not saying that they need to decide not to encapsulate after the considerations but just that they consider the points. When we discuss postpartum mood imbalances & disorders we need to look at a larger picture than just a placenta. We see many mothers of multiples who state they did not consume their placenta after baby #1 but did after baby #2 and felt better emotionally than the first time. However, did they review the other differences? Baby #1 we often know little to nothing about what the experience of mothering will really be like, we go at it alone, we are not very confident in what we already know and we hesitate to seek out much information. Often baby #1 was a longer labour and longer pushing stage. Going from no baby to a baby, no sleep, constant physical and emotional demands from the infant, plus ones own recovery can be overwhelming. Baby #2, labour might be drastically different, maybe this time more supported, a shorter labour, easier pushing, the lack of sleep one gets with a newborn in the house is not as much as a surprise and there is much more understanding of normal newborn behaviours. Maybe the second time she had a doula, the same lady who encapsulated the placenta for her, and also provided postpartum supports, like helping with baby care so she could nap or helped with dishes and laundry so mom can rest, put up her feet and just focus on breastfeeding. Having some healthy meals with nutritional elements similar to a placenta might be a more regular occurrence the second time. Speaking of nutrients; sometimes it is said that mammals consume their own placentas, so why wouldn’t humans? Some theories are that mammals do it for safety; that in the wild the smell of afterbirth would draw predators near and the mother & the newly born were vulnerable and at risk, so for safety, the mother would quickly consume the placenta. There are also some theories that a mother would be hungry and in the wild food is scarce. Their own placenta vs nothing was the best they could get so it could be considered a last resort for a nutritional deficient animal. We no longer live in the wild and food scarcity is not as prevalent. In this day and age, most humans don’t look at their placenta and see their next meal or have a desire to consume it. Even in the wild, they consume it mostly in one sitting and not small amounts over days and weeks like the placenta encapsulation community recommends now. Even with diminished nutrition in food sources, we can purchase vitamins and foods enhanced with vitamins, which could provide the same effects. There is a study I am aware of that is not yet completed and it does show that the mothers consuming their placentas do have higher hemoglobins at 6 weeks postpartum. However, it has also been commented that there is a chance that the families that have the available monetary funds to pay for placenta encapsulation services, also have the monetary resources to purchases better quality and quantity of foods. The cost of the placenta encapsulations has not been covered for the study. It is a control that needs to be considered. As a former Medical Laboratory Technologist who worked in manufacturing of blood and blood products, I also worry about an appropriate environment to encapsulate and I do have concerns about infection control. I know that might be over-reactive but as someone who had to do quality control, sterility checks and saw the process of recalls, I think safety and specifications are important. I mean, after all, the placenta might be contaminated with poop. Even a small amount of bacteria can cause a big tummy ache. I say that more tongue in cheek than anything, but it is a thought. There is equipment needed to encapsulate and I am just not 100% that the risk of cross contamination is not there. Now, I am not an encapsulator and maybe there are steps in place to account for that risk. I am unsure about that. I am just saying, for me, it is something to think about. In the lab, in food processing, in other areas where contamination is a risk, sterility checks and quality control is what keeps stuff “clean and safe” and where recalls start, if they are needed. Just because you made the organ does not mean it cannot hurt you if bacteria is at play. After all that, we do know that placebo effect can be strong and powerful. I am happy to accept placebo effect if you are and I am happy to refer you to a local placenta encapsulator if your desire is to encapsulate your placenta. This is a question the Pasqua South Medical Centre office staff often get asked when they make the recommendation to book an appointment with me. I am going to try and answer that question for you, and them. The centre staff may actually not know all the benefits of seeing me either. I am "new" to their space, they are getting used to me and gathering experience. They can see the improvements mom and babies are having, but they really do not know much about my services vs the free services. I bet it is safe to say that most people don't know the differences.
I am going to highlight a few. If you think of others that could be added, by all means leave a comment and I will add them in! 1) We, the client and myself, have a mutually agreed upon, prescheduled time. Free clinics often have you come in, take a number & sit and wait for your turn. They won’t likely know how many moms are going to show up, meaning mothers & babies (maybe fathers and other children,, too) could wait for quite some time and then be feeling rushed. They see all the other moms & babies waiting for their turns. At the centre we have a scheduled time, hopefully to your convenience and we allow enough time to avoid feeling rushed. Home visits provide a scheduled time AND the privacy and convenience of your own home. 2) I simply have more availability and flexibility. Not only is the timing better but you get more options as to when. Again, free clinics might only happen once a week. What happens if your struggles start on the evening the free clinic was being held and you missed it? Or sometimes you may benefit from two appointments only 2 or 3 days apart. A week can seem like an eternity when you are struggling. 3) I am an Internationally Board Certified Lactation Consultant (IBCLC). Not all the staff at the free clinics may be an IBCLC. The free clinics are staffed by Public Health Nurses (PHN's). Some PHN’s are IBCLC’s but not all are. I am an IBCLC dedicated solely to breastfeeding, with 10 years of experience helping moms and babies, 5 years as an IBCLC. (By the way, if you use the free clinic, don't hesitate to ask if the person helping you is an IBCLC. If you really wanted to, you could consult the IBCLC directory.) 4) Education is a high priority to me. I mean MY education and I mean YOUR education. I have attended, and continue to attend, a wide variety of additional & extended trainings and conferences. I have a strong ethical background to practice evidence based lactation “science”. I also want to give you enough information about what is going on with you and will answer all the questions you have. We book enough time to be able to do this. 5) In all my years of experience I have had access to ranges of breastfeeding from normal to extreme difficulties. My initial exposure to breastfeeding help was a peer-to-peer support group where our scope of practice was to help mothers by providing emotional support & information within “normal” breastfeeding. I got to know normal really well and be introduced to some not so "normal". I was super curious about those not-so-normal cases and pursued my IBCLC. Now I have much more training with the outliers of normal. I am also able to follow my own client cases much more closely to monitor outcomes and refine the plans along the way. This gives me the advantage to know whether the information and care plans I am sharing with clients really work. Often in a free/public setting you will be exposed to different staff member every visit and they do not have that same luxury. They might tell all the moms to do the same “thing” thinking it is best practice and not realize that is not useful for moms to do and they are not getting the desired outcome. 6) I have direct access to centre physicians if something is outside my scope of practice or comfort zone and we want or need a physician involved on some level. This is especially useful for further diagnostic testing or prescriptions we might want to consider. We have developed some great protocols together and collaboration like this is unique, yet so beneficial and much more efficient for resolutions of concerns. 7) It is my standard practice to do a through history of mother and baby. We need to make sure that we have all aspects and contributing factors considered when we are determining why there might be struggles. There are more factors to lactation than most people are aware of. I go much further beyond getting a better latch and a better position. We make sure to look at the situation from a few lenses. We pull out the puzzle pieces that might be problematic and piece by piece get the whole puzzle fitting together into a nice picture. You should hopefully be able to see what we are offering is completely different from what is being offered for free. You can count on focused, one-on-one care with a plan to approach the issues that brought you to me. You have the opportunity for follow up with the same person you saw originally and someone that can dialogue or report back to your physician and other care providers. I can help you address the specific concerns you have and reassure you what is the normal course of breastfeeding and give you my expertise with the more challenging aspects, with references and resources from the latest research. I can also make referrals and recommendations easily to a variety of other health care practitioners who may be of value to your specific concerns. I look forward to seeing all of you and your darling little ones. Please feel free to book an appointment at your convenience.  Disclaimer: I am not a mental health care professional or provider. If you think you are suffering from any sort of mental illness I recommend seeking medical attention as needed. I will also add in that I do take mental health concerns seriously and this blog post in not intended to down play medical concerns. Before you diagnose yourself with depression or low self-esteem, first make sure that you are not, in fact, just surrounded by assholes. - William Gibson When I first came across this quote, I immediately identified to it as an adult, as an individual and as I related to other adults. More and more I have been thinking about this in the context of my work, my work with new families, young babies and children & different relationships forming in homes. The rate of postpartum mood disorders is on the rise. Baby blues, anxiety, depression and psychosis are a very real reality for many new mothers and fathers. We mostly see it in the context of mothers but more and more research shows our fathers are impacted by mood disorders as well. Let’s, however, just step back for a minute and think about the above quote. “Before you diagnose yourself with depression or low self-esteem, first make sure that you are not, in fact, just surrounded by assholes.” I don’t want to be rude but let’s face it, babies are assholes, toddlers are assholes and kids can remain like that as they grow up. They certainly don't mean to be but they are incompetent & demanding, they can be obnoxious and rude, they interrupt your every meal and all your sleep. You can’t even think about peeing without baby waking up and crying, let along move an inch to try to get up and pee. They need to be fed constantly, hanging off your breast, YOUR breast no longer belongs to you. When they are not feeding, they need you to hold them or they will turn the reddest of red and blow horrible smoke from their ears. They pee and poop ALL.THE.TIME. Rudely, they sometimes don't even wait for the new diaper to get on before they shit all over you or shower you in pee. You imagine stuffing that thing back inside you, because as awful as it was to have that watermelon come out the lemon, they are way easier to take care on the inside, right? Well, too bad, there is no turning back. There is only moving forward with this asshole in your life. By now you know I am not serious in calling babies assholes, but you can see my point. Life is HARD with a new little person to care for. The real assholes of the world are hard enough to put up with, but now you have to put up with the smallest of them all, ALL the time, because YOU created it after all, YOU wanted this. Now you have to do it when you have zero sleep, zero nutrition and probably zero clue how to actually take care of this baby - I can guarantee you it did not come with a manual. Add in some hormones and everyone’s opinion of what you should be doing and it is easy to see why one would end up with signs and symptoms of a mood disorder or postpartum depression. So, how about we get serious about what we can do about this baby and get through what will be one of the most challenging times of your life. Self-care is big. You don't want to lose yourself in this. Having a baby WILL change you, but doesn’t need to consume you. What do YOU need? What does your partner need? Make a plan to have that happen. 15 minutes in the shower, making two sandwiches instead of one when your partner leaves for work, tea out with friends. Asking friends to bring you food when they come visit the baby. By the way, when they come visit, the asshole will switch personalities and put his nice guy face on. Have someone come help with light house work and laundry once a week. It’s the small things that make a massive impact. Communication is huge. Tell each other how you are feeling about the changes in life and the new demands. If you are reading this before having your baby, start that conversation now. Brainstorm the different ways to achieve self-care that will work after baby. Be open and flexible in changing those plans, if needed. Just talk to each other and others about what is happening in your new world. Just keep the conversations going. And find others who will listen to you both. Just someone who will let you get it out. I promise, they won't mind. Support. SUPPORT. SUPPORT. This is a must. You need to build a team of support people. Before baby is ideal but may not have happened and you may now just be building a support team. Who are we talking about? Family, friends, community resources - your health care providers, doula’s, peer support groups. Everyone’s team is going to look different depending on the needs they have. What is important to know is that support is going to make one of the largest impacts in how you feel about everything and how stable your mood will be, how you will interpret your experiences and what the outcome of the situation is. It is important to identify your needs and equip yourself with the tools to get there. It is vital to know what your support options are because without options you have no choices. So, start now by identifying your needs and making a list of supports. If you get lost and have a need but don't know how to get the support you need to have that need met, please ask! I am here to help in this time of transition in your life. |
Kim Smith
|
 RSS Feed
RSS Feed

|
|
Lactation Consultant (IBCLC)
Serving Regina SK & Area 306-550-6143 kim@kimsmith.org Quick facts:
International Board Certified Lactation Consultant (2010), Re-certified (2015, 2020) TummyTime Method Instructor Retired Doula, CAPPA trained, Pre-Certified ProDoula (2009) Your Birth Experience (YBE) Certified (2015) Wife & mother of 4 Retired Medical Laboratory Technologist |